Frequently Asked Questions
No. The DXR+ has to be irradiated from the printed X-ray arrow and with a continuous field to give a correct result.
The VT305 is optimized for battery use. Ensure that the battery is fullycharged. The VT305 will operate on battery power for up to four hours ofcontinuous use. Shorter battery life will be experienced when the VT305 iscommunicating with computer applications such as the browser-viewedconfigurator, etc.
On the base unit side, use the Bluetooth device with USB connection that is provided by RaySafe (Laird BT820, pn: 1922064).
On the computer side there are various reasons for unstable Bluetooth connection such as incompatible hardware/software or environmental radio disturbances during measurements. Try turning off any programs on the computer that may interfere with the Bluetooth connection.
If the problem persists, you can try using a RaySafe Bluetooth USB device on the computer side as well. Turn off the internal Bluetooth.
Dose Manager is a software installed on your PC to see the history of dose exposures. You can see a dosimeter’s exposure over time and compare it to other dosimeters. With Dose Manager, you can also collect dosimeters exposure history from the Real-time Display and do not need to connect them individually to your computer. Dose Viewer compared to DoseManager can only show information for one dosimeter at the same time, and the dosimeter must be connected directly to your computer when you look at the history.
- No, i3 badges are not legal dose of record. The readings they record should be used for reference and behavior modification.
Remove the luminance tube and ensure that the white illuminance window is clean. You can clean it with a damp cloth. If the problem persists, fill in a Service Request and send the detector for service.
I have connected the mAs cable but don't get any readings. What can I do?
The fastest way to charge the base unit is to use the supplied charger. You can also charge with USB cable connected to a computer or a USB charger, but this will take longer.
The i3 has improved wear-ability with a replaceable reinforced plastic clip. The i2 had a metallic clip that could not be replaced.
No, the dosimeter is designed for maintenance-free usage throughout its lifetime.
- When the instrument is in measurement mode, press SELECT (long press) until "Waiting... Aborting measurement" is shown.
- In the SETUP MENU, step (short press) to "Dose unit" and press SELECT until units are shown. Step to the desired unit and press SELECT until SETUP MENU is shown. The unit is now changed.

Note: If only Gray (Gy) is available, your instrument has been configured to comply with German regulations where the unit Röntgen (R) is not allowed.
The VT305 can be connected to mains power using the universal poweradapter and the appropriate prong-set (matched to the mains powerreceptacle). The power adapter connects to the VT305 via the USB cable.Alternatively, if a computer is being used during testing or documentation,you can connect the VT305 directly to the computer via the USB cable. Bothpower and data exchange are provided.
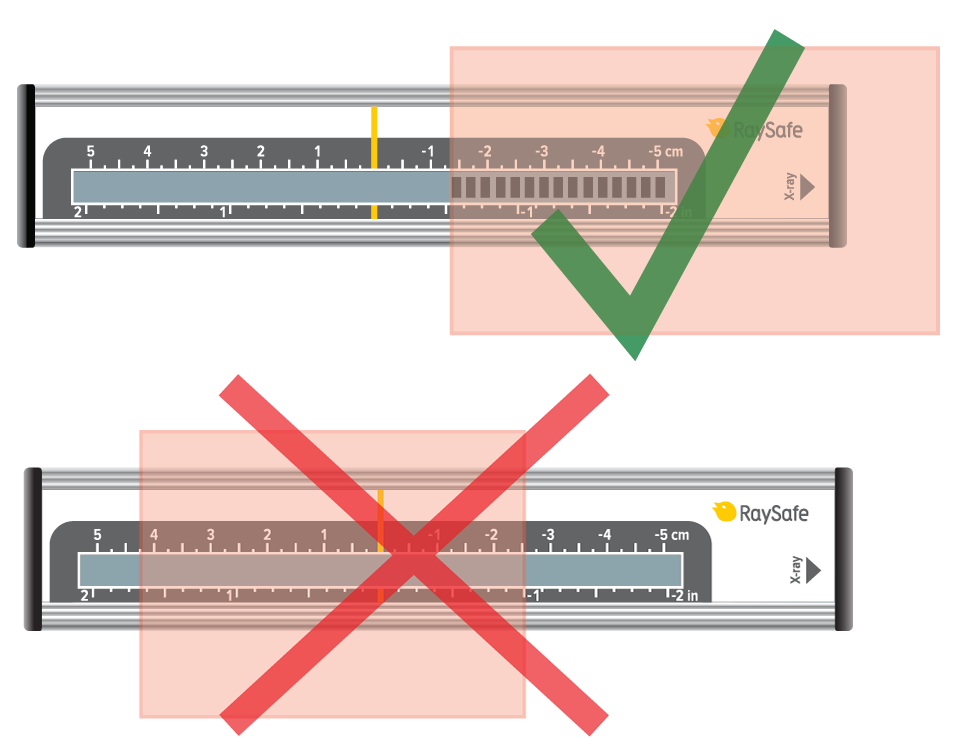
Panoramic dental machines can be challenging to measure on, primarily since the X-ray beam is narrow. Therefore, the positioning of the active sensor area is crucial.
Use DENT or R/F sensor.
Position the sensor in the exact center of the X-ray field, where you have the highest dose.
The positioning can be sensitive down to 0.1 mm. Use the RaySafe X2 panoramic holder to slide the sensor horizontally with high precision. Each mark on the scale represents 0.2 mm.

For details on how to use the panoramic holder, see the instruction video in our video library.
Dose Manager can be used with the new i3 dosimeters if you collect the dose information from your Real-time Displays using a network connection or with a USB memory. The i3 dosimeters unfortunately cannot currently be connected directly to Dose Manager by the USB cable.
- No, the feedback is visual. Because of this, it is best for the Raysafe Display to be located in an easily visible location for the staff.
Check that the cable is properly connected. Try another cable.
Swipe right from the home screen to access the setup. System language is found under X2 Base Unit. You will be asked to restart the base unit for the setting to take effect.
The i3 has room for naming, whereas the i2 does not.
The RaySafe Real-time Dosimeter: Approximately 1 year of normal use. The battery can be replaced. See the Installation and service manual for guidance.
The RaySafe i2 dosimeter: Typically 3-5 years, depending on usage. If the battery is out, contact your RaySafe representative or RaySafe Support Contact.
R/F high can be used for most measurements and is required for measuring kVp (as opposed to kV).
R/F low is optimized for low radiation intensity, typically during fluoroscopy measurements behind a phantom.
Use the VT305 with the Ansur VT Plug-In. You can use either a ready-for-usetest procedure or drag and drop one or more test elements from the Plug-Inonto the test template workspace in the Ansur software authoring screen(see Ansur Executive Operators' Manual for more information).Questions and Answers6045 Cochran Rd, Cleveland, OH 44139 USA | Tel 440.248.9300 | Fax 440.349.2307 | Email: [email protected] | www.flukebiomedical.com
The Dose Viewer version 1.1.13.0, delivered with the RaySafe i3, is backwards compatible with the RaySafe i2. Older versions of Dose Viewer need to be updated to support i3 Real-time Dosimeters.
The default Excel export format in X2 View is compatible with Xi View.
Unfortunately, this is not possible with the RaySafe i2/i3. This is something that we look in to for the future but currently only the Real-time Display can be used to visualize the exposure situation in real time.
- i3 badges will enter sleep mode after 9 minutes of not detecting any movement.
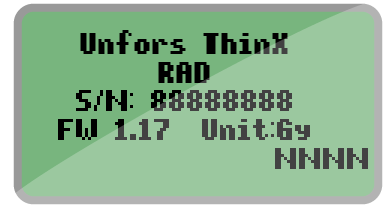
- If you just replaced the battery, this means that your ThinX is starting up. Be patient and wait for a while.
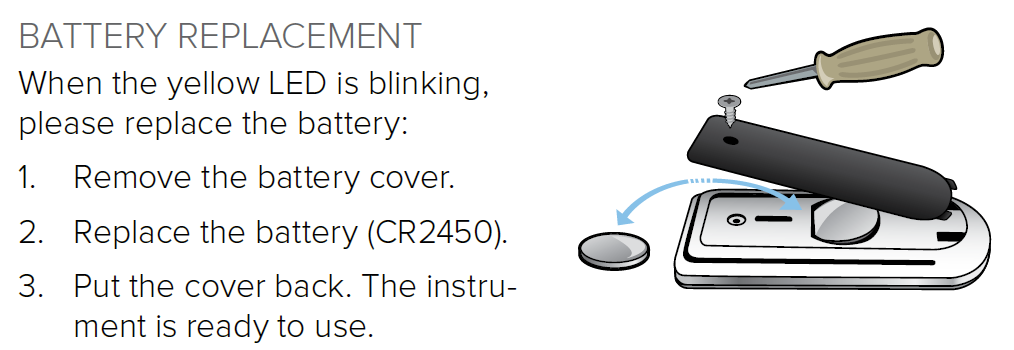
- If the screen appears when you are exposing the ThinX to radiation, you need to replace the battery (model CR2450). Follow the instructions in the user manual: ThinX RAD or ThinX Intra. We recommend using a battery from GP Batteries.
- Check that you are running the latest version of Xi View and remove older versions from your computer.
- During installation, make sure to tick the box "Install Windows 8 USB driver for serial port adapter".
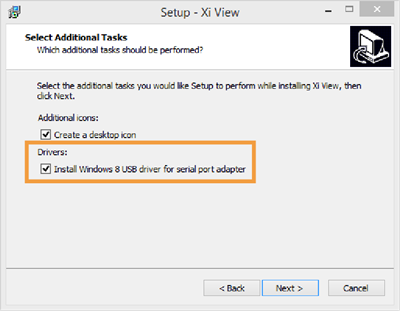
- In Xi View, select "ATEN USB to serial bridge" in the lower right corner. You may need to re-select it.
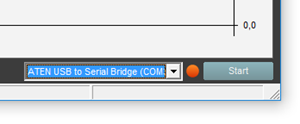
- In Xi View, press the "Start" button in the lower right corner and wait until the dot beside it turns green.
- If you have a Solo instrument, check that you have the RaySafe Solo PC kit.
Note: If your Solo instrument came with serial cable and usb-serial converter, it has the PC kit. If you wish to add the PC kit, contact Customer Service.
Swipe right from the home screen to access the setup. Press the name of the currently connected sensor to find the unit setting.
Note: If only Gray (Gy) is available, your instrument has been configured to comply with German regulations where the unit Röntgen (R) is not allowed.
Yes, they can, i2 and i3 dosimeters will show up on DoseAware base station screens and DoseAware dosimeters will show up on the i2 and i3 base stations screens. As the icons used for dosimeters are not the same for i2/i3 and DoseAware, the dosimeters might however appear differently.
To access the dose history recorded in the Real-time Display, tap on the row for your dosimeter on the display.
To access the internal dosimeter memory, connect the dosimeter to a computer running Dose Viewer.
The RaySafe Xi calculates kVp on the R/F high sensor if the intensity is high enough (around 10 mGy/s), otherwise kV average will be displayed. If the intensity is too low and you have no possibility to increase the tube current (mA), move the detector closer to the X-ray source.
Note: If your signal level is well above 10 mGy/s and you still do not get kVp, go to the SETUP MENU, select kVp mode, and make sure that kV/kVp is selected.
The VT305 uses a single measurement channel for all gas flow assessments.The display's (numeric and waveform screens) are auto-scaling and autorangingfor simple connection and use.
The RaySafe i3 has a customer replaceable battery, which prolongs the product life cycle up to 10 years. The RaySafe i2 badge needs to be replaced when the battery ends in <5 years.
Yes, all common mammography machines are supported. Just connect the X2 MAM sensor and measure to get dose, HVL and time on any beam quality. If you also want the tube voltage (kVp), you must select an anode/filter combination. Swipe left from the home screen to select.
Take a look in the Mammography coverage table to see which anode/filter combinations the X2 can give a kVp value for.
Yes, additional badges are available for purchase.
- Yes, i3 badges can be set to stay on all the time. This will drain the battery faster, however.
Read "SETUP OF BLUETOOTH COMMUNICATION" on page 6 in the Xi View User Manual. If you have established the Bluetooth communication as described in the User Manual but still have problems, try turning off any programs on the computer that may interfere with the Bluetooth connection. On the computer side, there are various reasons for unstable Bluetooth connection such as incompatible hardware/software or environmental radio disturbances during measurements.
Position and measure as usual. The X2 has full AMX4+ support.
Please visit www.RaySafe.com/i3/downloads, download and install the latest Dose Viewer that support i2 and i3 dosimeters.
No, the intended use for the i3 and i2 systems are to measure scattered radiation only.
It is enough to measure kV for one beam quality per machine, since the set kVp is independent of anode material and filtration. The Mammography coverage table lists what you can measure on different machines.
The Compliance parameter shown on the FULL (full test) numeric display ofthe VT PLUS is a dynamic value calculated from tidal volume and pressurevalues breath-by-breath. The Cstat parameter shown on the VT305 is a staticcompliance parameter calculated using the formula Cstat = VT / (Pplateau -PEEP) where Pplateau is the Inspiratory Pause Pressure. Not all ventilatorsprovide an inspiratory pause/hold function. If there is no plateau pressure,the VT305 Cstat displays"---" since a division by zero would result.
The EMC immunity in the i3 has been significantly improved over the i2, reducing possible interference.
Real-time measurements from up to eight dosimeters are shown simultaneously on the screen. The i3 has a sleep mode so only active dosimeters user show on the screen. The i2 dosimeters are always on and shown on the screen when in range.

Display: Luminance mode. For contact measurements on a display or view box.
0: Zero adjustment.
Light bulb: Illuminance mode. For measurements of ambient light or intensity from a collimator lamp.
- Prolonged life cycle
- improved EMC immunity
- better measurement specifications
- automatic sleep mode
- improved wearability.
The DXR+ works well placed on the examination table. Use as high kV as possible.
Note: Do not position the DXR+ on top of a magnification table, since the signal is too low there.
CRC error means that part of the data has been lost or altered in transit. This can happen when the distance is too long, or if something is interfering with the signal. Create a clear line of sight between the base unit and computer, or use a shorter distance.
Press the desired parameter from the home screen to go to full screen mode, then swipe left for the waveform. Waveforms are available for kVp, dose rate and mA.
Yes, you can.
Place your CT detector on a flat surface and restart the base unit. Do not touch or move the detector. If the "Stabilizing" message does not disappear within 5 minutes, fill in a Service Request and send the detector for service.
To save measurements press and hold the "O" button at the upper rightcorner of the VT305 display until the "Data saved toDATAxx.CSV" message is displayed on screen. This meansthat the measurement values have been saved to the microSD card in the VT305.
The i3 measurement performance is an improvement over the i2, and includes angular reception making it more accurate.
The real-time display can be installed anywhere, it only needs a power outlet (network connection is optional). The dosimeters communicate with the display via radio. The radio communication range depends on the local environment and the Real-time Display settings (Service Manual) but is normally about 5-15 meters.
The X2 Base Unit can store several thousands of measurements.
- Swipe down from the home screen to see previous measurements.
- If the base unit has been turned off, or if you have switched to a different sensor, look in the measurement archive: Press the menu button and then Measurement archive. Select the session you want to take a look at.

- You can also use X2 View on a computer and select Import from Base Unit in the File menu and select from the calendar. See the X2 View manual for more details.
No, you have to send it to RaySafe for battery replacement. Fill in a Service Request to get it done.
To update firmware in the VT305 do the following:1. You will receive an update file (e.g. filename C0204000.S19) fromFluke Biomedical.2. Remove the micro SD Card from the VT305 and insert the card into your PC.3. Copy the update file onto the microSD Card.4. Remove the micro SD Card from the PC.5. Insert the micro SD Card back into the VT305.6. Restart the device (power on the VT305).7. The screen will show you the update's progress8. When the update is finished, the device will restart by itself.
The user manual for X2 is called "Help" and is integrated in the base unit. Press the menu button on your base unit and then "Help" to see the user manual for your system. You can also find video tutorials and pdf-manuals on the Product support page.

Yes, can combine i2 and i3 badges but be aware that measurement results may differ. We recommend that you replace the i2 badges with i3 ones as soon as possible to increase the efficiency of your RTSD.
Offset out of range is shown when the current in the ionization chamber fails to reach a stable level. Please make sure that:
the chamber is not irradiated during the stabilization or zero adjust phase, you are operating the instrument within its specified temperature range (15-35 °C).
If the problem persists, fill in a Service Request and send the detector for service.
I get too low readings with my Light detector. Why?
To retrieve measurements from the VT305 micro SD card:1. Remove the micro SD card from VT305 andinsert it into the appropriate SD card adapter(provided as a standard accessory with theVT305).2. Insert the micro SD card and SD card adapterinto the SD card reader, or insert the micro SDcard into the USB SD card adapter (providedas a standard accessory with the VT305).3. Connect the SD card to a computer.Questions and Answers6045 Cochran Rd, Cleveland, OH 44139 USA | Tel 440.248.9300 | Fax 440.349.2307 | Email: [email protected] | www.flukebiomedical.com4. Open the SetupReportFormatter.bat file fromthe VT305 micro SD card. This file has a macrothat imports data into your computer from theVT305.5. Open each .csv file in the DATA folder on themicro SD card. When a .csv file is opened, adialog box shows in the computer display andasks whether the data should be formatted.6. Click €˜Yes' to make a formatted report file. TheVT305 test report, like the one shown at theright, will be created.7. The .csv file can also be opened in anunformatted form using Microsoft™ Excel™.Click €˜No' and an unformatted .csv file will bedisplayed. The data can be formatted asdesired.NOTE: The files on the VT305 micro SD card cannot be renamed.
No, the i3 does not use a cradle like the i2. The improved i3 design lets you just use a USB cable to connect the dosimeter to the computer.
The dosimeter always measures and stores dose data on its internal memory, regardless of whether there is a display in range or not. You can view the dose history at any time by connecting the dosimeter to a computer running Dose Viewer.
To see the dose rate live, the dosimeter needs to be visible on a real-time display. The dosimeter shows up on any Real-time Display within communication range, it is not paired with a certain display.
The region inside the dashed red line is the active sensor area.
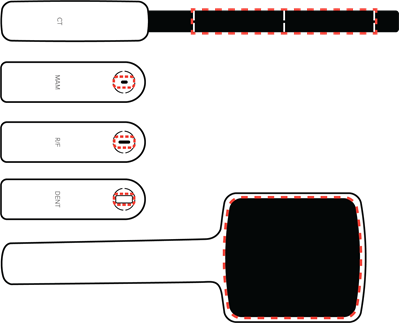
Note: Keep the active sensor area and its surroundings clean and free from stickers. Added material in the X-ray field may affect the measurement result.
Yes and it is standard on all TNT 12000 systems.
One. All measured parameters (kV, dose, time, HVL) are displayed all the time with each exposure, saving valuable setup time. Because TNT 12000 always defaults to the previous settings when powered down, many repetitive QA and calibration routines can be set up and completed by the stroke of a single on/off key.
Bluetooth wireless technology has several disadvantages that ZigBee does not. First, when turning on a Bluetooth-equipped device, the transmitting unit will search for available receivers and present a list from which the correct device must be selected. ZigBee units are paired, so upon scanning for detectors one does not get every wireless device in the local area, but only those ZigBee units paired with the companion TNT 12000 display or computer. Also, the power output is lower so ZigBee does not interfere with nearby medical devices, and greatly extends battery life of both display and detectors.
With the TNT 12000 solid-state detector or DoseMate dosimeter set to fluro mode, position either detector with the measuring side facing the X-ray tube at the prescribed distance from the focal spot. Completely block the image receptor using copper or lead sheets and begin the test.
TNT 12000 solid-state detector is slightly lower in accuracy (but much smaller, wireless, and easier to use than the Keithley Triad), and the DoseMate/ion chamber combination is equal to or greater accuracy compared with the Keithley Triad (both use the same ion chambers).
No, the 35035 is a standalone unit. The TNT12000 and the DoseMate dosimeter are both upgradable to include mA/mAs measurement functionality. These upgrades allow mA/mAs measurement values to be included in the diagnostic X-ray information displayed.
Both the Excel add-in and Ansur Test Automation software automatically capture test data and facilitate data management and reporting. The Excel add-in collects measured values and populates a customizable Microsoft Excel spreadsheet template; A MQSA-specific template is included for Mammo applications. Ansur provides a visually-guided inspection procedure that reduces human error with step-by-step visual instructions, auto-configuration of compatible test instruments, auto-data collection of measured values from compatible test instruments, auto-comparison of measured values against pre-determined test limits, and objective determination of Pass/Fail. All inspection results are included in a single, test result file and customizable test report that can be printed or stored digitally. Ansur Test Automation software is also compatible with a range of CMMS software systems. All users may utilize the Excel add-in for reporting purposes. Users who need to standardize testing and reporting procedures (especially when performed by multiple associates) and minimize risk of human error benefit from Ansur Test Automation software.
Turn Auto-reset OFF and the DoseMate electrometer will accumulate dose values. Turn Auto-reset ON to allow the DoseMate electrometer to reset between exposures.
Each of the two sets of cross-hairs on the TNT 12000 solid state detector are marked as to their use. The gray-colored cross-hairs are for Rad/Fluro, while the red-colored cross-hairs are for Mammo. These aid in centering the detectors in the X-ray beam
Yes it is possible to perform kV and other X-ray tube parameter measurements for the standard dental X-ray tube (TNT12000WD may need to be attached to a camera tripod to hold it in place in the beam.) Panoramic dental X-ray, like other modalities where the X-ray tube is rotating/moving, requires the tube be kept in place (not moving) to measure X-ray tube parameters. If dose is the parameter of interest, use DoseMate and an appropriate ion chamber capable of detecting X-ray energy in a 360 o arc about its center. There is no special calibration needed in either case.
Use the DoseMate and the 15 cc ion chamber in the table Bucky tray to obtain time measurements.
Any firmware or software upgrades that do not affect calibration of the TNT 12000 are available on the Fluke Biomedical website under Support: Software Downloads.
There are two options.
- Standard: Mo/Mo for Mammographic and W/Al for Diagnostic-standard calibration
- Optional: Mo/Rh, Mo/Al, Rh/Rh, Rh/Al for Mammographic
No. One should pick the data-collection and display device that best meets the needs of particular application scenarios. For example: 1st call triage of reported X-ray system problems might be best managed using the TNT 12000 display unit and the appropriate detector or combination, while scheduled inspections or calibration might best be served by an Ansur visually-guided inspection procedure, or an assessment of image quality vs. dose might best be served by the DoseMate/Excel Add-in combination.
No. The display unit will work with any TNT 12000 solid-state detector or DoseMate.
Use the TNT 12000 solid state detector in Fluro-mode.
PPV means practical peak voltage and is a measurement used outside the USA for assessing X-ray tube performance.
No. The TNT 12000 display shows only the last measurement. If measurements need to be saved, the Excel Add-in is recommended. If both measurements and other inspection results in an overall inspection procedure need to be saved, then a visually-guided inspection procedure should be created using the Ansur TNT 12000 Plug-in. This inspection procedure documents the entire process and all inspection results (physical/visual inspection, mechanical inspection/adjustments, electronic measurements, lubrication steps, replacement of consumable items, etc.)
A minimum of 500 mR/min doserate is needed to get accurate kV results.
There are five different possibilities:
- Blue - Display or detector is connected to a power source and the battery is fully charged.
- Green - Display or detector is connected to a power source and the battery is charging.
- OFF - Display or detector is not connected to a power source and is operating on battery power.
- Yellow - Display or detector battery has approximately 20% of charge left.
- Red - Display or detector battery has approximately 10% of charge left and will turn off in two minutes.
A 15 cc ion chamber is useful for Radiographic X-ray systems and Mammographic X-ray systems; a 150 cc ion chamber is useful for Flouroscopic X-ray systems (e.g., input dose to image intensifier), Scatter assessment, and any situation where the increased sensitivity of the chamber allows measurement of lower dose-rates.
The waveform is accurate enough to assess whether there are problems in the X-ray tube or generator not disclosed by the numeric measurements. To obtain more accurate waveforms or to perform calibrations using the waveforms the 35080M199 X-Ray Scopemeter is recommended.
Yes. The IEC 61674 is about dosimeters with ionization chambers and/or semi-conductor (solid-state) detectors as used in X-ray diagnostic imaging and contrary to other kVp meters in the Fluke Catalogue the TNT12000 is compatible to this European Standard.
TNT 12000 uses a proprietary multi-element solid-state detector that simultaneously measures the variable attenuation experienced by adjacent elements to determine the HVL with just one exposure.
The TNT 12000WD was performing an internal amplifier nulling process but detected a start of X-ray shot and gave an error message.
Ion chambers can be added to the DoseMate using the Display, through the Excel Add-in, or with Ansur software.
Monophasic waveforms used in the legacy defibrillators, biphasic waveforms in most of today's technology, as well as pulsed biphasic waveform, an emerging new technology.
- Age of battery pack. The battery pack will lose some charge capacity over time.
- Use of the backlight display function. This option discharges the battery pack faster.
- 3. Operating the unit at the upper end of the specified operating temperature range, causing the internal fan to power on more often. This may especially be observed with multiple, rapid, high-energy defibrillator pulse discharges into the unit.
Sampling rate should be 5 times the X-ray system frequency for accurate kv waveform analysis. The GE AMX4, the most ubiquitous mobile in the world, operates at 2 kHz. Systems like the Unfors Xi and RTI Piranha sample at around 2 kHz and thus cannot adequately sample an AMX waveform.
If the Impulse 6000D/7000DP is turned on, make sure the "Charge Battery" setting is set to "Yes" on the "Set Up: Battery" screen (refer to the operating manual for details). If the Impulse 6000D/7000DP unit is turned off, the LED should glow red when the external charger is connected correctly and mains power is present.
The SigmaPace1000 is designed to test external cardiac pacemakers only. The two compatible types of external cardiac pacemakers are these:
- Transcutaneous: This type of pacemaker (typically built into a cardiac resuscitation unit with a defibrillator) has output currents ranging from 30 to approximately 200 mA. External adhesive electrode pads are attached across the patient's intact chest to deliver the energy. (The Impulse 4000 also tests this category of external pacemaker.)
- Transvenous: This typically small handheld unit, powered by a single 9-volt DC battery, generates pacing pulses at levels from 1 to approximately 25 mA. This type of pacemaker is available in many different configurations from simple single chamber models to more sophisticated AV sequential dual chamber models. The pacing electrodes are introduced via the patient's venous circulatory system via a temporary indwelling cardiac catheter connected directly to the heart.
Plug the battery charger accessory included with your analyzer into the charger input on the rear panel and plug the mains cord into the charger unit and into mains power. The charge-status LED, visible from the rear panel, will glow red to indicate the battery is charging. The LED will turn green when charging is complete. A full recharge takes approximately four hours or less.
The basic difference is the direction of current flow between the defibrillation pads. With a monophasic waveform, the current flows in only one direction. With a biphasic waveform, the current flows in one direction, then reverses and flows in the opposite direction. Lower energy is used in biphasic waveforms.
No. For safe and reliable operation, the battery charger MUST have a good earth ground when connected to the Impulse 6000D/7000DP, and vehicle electrical systems inherently lack an earth ground. For battery charging only (with the Impulse 6000D/7000DP turned off, and no other connections to the Impulse 6000D/7000DP unit other than at the charger input jack), using a DC-to-AC inverter to power the battery charger may yield consistent battery charging, depending on the quality of the inverter used. As of this writing, Fluke Biomedical cannot recommend the use of a DC-to-AC inverter for battery-charging-only use with the Impulse 6000D/7000DP.
Ensure the solid state detector is facing the tube and is perpendicular to the X-ray tube axis. For under-table tubes, this means that the solid state detector should be placed face-down on the X-ray table.
When combined with the high-end functionality improvements of the Ansur test automation system, your Fluke Biomedical analyzer provides a solution-based approach to complete analysis of the medical device under test. Fluke Biomedical test equipment with Ansur automation solutions create standard work using test templates/sequences based on customer's written test procedures, manage test procedures by allowing both manual and visual automated test sequences, and integrates all test results into a single test report, which can be printed or archived.
No! The SigmaPace1000 dual channel input jacks on the SigmaPace1000 are protected against an occasional application of a high-voltage defibrillator output. The analyzer's protection circuitry is designed to withstand accidental discharges at 360 J.
No. For safe and reliable operation, the battery charger MUST have a good earth ground when connected to the Impulse 6000D/7000DP, and vehicle electrical systems inherently lack an earth ground. For battery charging only (with the Impulse 6000D/7000DP turned off, and no other connections to the Impulse 6000D/7000DP unit other than at the charger input jack), attempting to charge from a 12 V vehicle gives inconsistent results and therefore cannot be recommended.
No. Different waveforms perform differently depending on their shape, duration, voltage, current, and response to impedance. Different biphasic waveforms are designed to work at different energies. Impulse 6000D/7000DP measures the monophasic waveforms used in the legacy defibrillators, biphasic waveforms used in current technology, as well as pulsed-biphasic waveforms, an emerging technology.
No. Replacement of the battery pack in the Impulse 6000D/7000DP requires disassembly of the unit. Impulse 6000D/7000DP owners who send their units to a Fluke Biomedical Authorized Service Center for periodic calibration may want to consider requesting replacement of the battery pack as preventative maintenance, which can be performed for a nominal charge.
Cables require time to set up and put away after use, which reducess, and can be bumped or stepped on during operation-causing erroneous readings, delays and other productivity challenges.
Impulse 7010, Defibrillator Selectable Load Accessory, in conjunction with Impulse 7000, Defibrillator/External Pacer Analyzer, is specifically designed by Fluke Biomedical to allow defibrillator manufactures and end users to comply with portion of IEC 60601-2-4 and AAMI DF80 standards.
Impedance in humans has been shown to vary anywhere from 25 to 180 ohms with the average impedance of an adult around 70 to 80 ohms according to an AAMI study. A well designed defibrillation waveform must measure patient impedance and adjust the waveform shape and duration accordingly to optimize waveform performance across the range of anticipated impedance values.
The "Section 6.8.3" of the IEC 60601-2-4 standard and AAMI DF80 standard require defibrillators to be tested on different resistant loads of 25, 50, 75, 100, 125, 150, and 175 ohms to ensure proper energy is delivered to patients with different impedances. Impulse 7010 is also the only testing tool to test defibrillators beyond 175 ohms. A 200 ohms option gives manufactures the capability to test defibrillators under extreme impedance conditions. In addition, interface with Fluke Biomedical Ansur, PC-based automation software, allows for standard, streamlined and time-saved operation and total digital data management.
Use of Impulse 7010 is easy. Simply connect the Impulse 7010 output connectors to the input connectors of Impulse 7000 as shown in the figure below. The various connection combinations available through the Impulse 7010's rotary switch provide eight different loads for a defibrillator discharge.
Yes. Actually, to keep the reported battery charge level as accurate as possible during extended periods of non-use, it is recommend that the Impulse 6000D/7000DP be left connected to mains power via the battery charger with the unit powered off, in an ambient temperature of 15° C to 26° C (60° F to 78° F). This will continuously trickle-charge the battery (the charge-status LED on the rear panel will be green) to keep both the actual and estimated battery charge level at 100 %.
If the Impulse 6000D/7000DP cannot be kept connected to the battery charger during periods of non-use, the battery should be charged at least once a month. A unit with a discharged battery that is stored for an extended period of time will result in the battery becoming over-discharged, which is likely to result in permanent damage to the battery.
Impulse 7000DP tests the full function of transcutaneous pacers, but not transvenous pacers. For transvenous pacer testing, try the SigmaPace 1000 or DALE400 analyzers.
No. For safe and reliable operation, the battery charger supplied with the Impulse 6000D/7000DP MUST be used when operating from mains power, or when operating and charging the battery at the same time.
A minimum of 500 mR/min doserate is needed to get accurate kV results.
The fan on the back of Impulse 6000D/7000DP is controlled by a thermostat IC. The thermostat utilizes an on/off control (i.e., not linear or continuous control). The thermostat IC is located next to the defibrillator load resistor.
There are two temperature thresholds. The lower threshold is set at about 40° C (104° F) and the upper threshold is set at about 50° C (122° F). When the temperature exceeds the low threshold, the fan turns on. When the temperature exceeds the upper threshold, a warning message is displayed and the unit will not make any further measurements until the temperature has dropped below the upper threshold.
On the Impulse 6000D/7000DP, the internal battery pack contains a gas-gauge IC that monitors the battery-charge level. This gas-gauge IC reports the charge level as one of sixteen levels, from 0 % to 100 %. The Impulse 6000D/7000DP reports the battery-charge level in 5 % steps, from 0 % to 100 %. Therefore, five of the 5 % steps aren't used (15 %, 35 %, 50 %, 70 %, and 90 %). The "Power = 50%" message is an indication that the microprocessor was unable to communicate with the battery pack. If this message persists, the battery pack is probably defective.
When combined with the high-end functionality improvements of the Ansur test automation system, your Fluke Biomedical analyzer provides a solution-based approach to complete analysis of the medical device under test. Fluke Biomedical test equipment with Ansur automation solutions create standard work using test templates/sequences based on customer's written test procedures, manage test procedures by allowing both manual and visual automated test sequences, and integrates all test results into a single test report, which can be printed or archived. Biphasic Monophasic
No. The Impulse 6000D/7000DP was designed and tested to meet all its performance specifications at any battery-charge level when operating from mains power or when operating from mains power while charging the battery.
ZOLL M Series and PD14000 use different algorithms to output pacing function. The default ZOLL MEDICAL pacer selection in Impulse 7000 uses ZOLL M Series algorithm to detect pacer output from ZOLL pacers. We recommend that customer choose ZOLL MEDICAL brand under Impulse 7000 PACER testing function when testing ZOLL M Series, but choose DEFAULT ALGORITHM when testing ZOLL PD14000 to get accurate readings.
Select the manual waveforms icon in the Excel Add-in tool bar and then select the waveform (and how much of the waveform) to be viewed.
This is not necessary. The battery does not exhibit a "memory effect". After multiple partial charge-discharge cycles, or if the unit is unused for an extended period of time without the charger active, the battery level indication may become inaccurate (i.e., out-of-sync with the actual battery charge level). Completely discharging the unit before charging it will resynchronize the battery charge level indication.
No. The SigmaPace1000 was designed to test a wide range of external pacemaker parameters. It is not intended for use with internal pacemakers. Manufacturers of internal cardiac pacemakers offer sophisticated test systems that are designed for their specific brand and range of available internal pacemaker models. These test systems typically perform specialized functions such as tissue impedance measurement, and also program operational parameters of these implantable cardiac pacemakers. These diagnostic test systems are utilized during surgical implantation procedures and have direct contact to the patient's heart.
ZOLL M Series and PD14000 use different algorithms to output pacing function. The default ZOLL MEDICAL pacer selection in Impulse 7000 uses ZOLL M Series algorithm to detect pacer output from ZOLL pacers. We recommend that customer choose ZOLL MEDICAL brand under Impulse 7000 PACER testing function when testing ZOLL M Series, but choose DEFAULT ALGORITHM when testing ZOLL PD14000 to get accurate readings.
The Impulse 7010 only works with Fluke Biomedical's newest defibrillator/external pacer analyzer, the Impulse 7000DP. It will not function with legacy Fluke Biomedical analyzers such as Impulse 4000, QED6, QA40/45, or with competitor products.
Yes. The manufacturer of the NiMH battery cells used in the Impulse 6000D/7000DP specifies a typical loss of 10 % of battery charge after 500 charge-discharge cycles, which is approximately two years of daily use. Battery charge capacity also degrades with time, so even a seldom-used unit will lose some battery charge capacity. The Impulse 6000D/7000DP battery power feature was designed conservatively to maximize the probability of the battery pack performing satisfactorily well beyond two years.
The answer to this question is somewhat counterintuitive. Battery pack gas-gauge ICs, such as the one used in the Impulse 6000D/7000DP, use a complex algorithm to estimate battery-charge state, taking into account time, temperature, and current flow. The self-discharge estimation (i.e., how much charge the battery loses over time during periods of non-use, sometimes called "shelf-life") is particularly sensitive to battery chemistry, and the shelf-life of today's NiMH cells is significantly longer than the algorithm built into the gas-gauge ICs can accommodate.
When an Impulse 6000D/7000DP is left idle for a few weeks and then powered-on, the battery charge level might be reported as 55 % when the true charge level might be 80 %. If the battery is then completely charged, which requires a 20 % increase in battery charge level, the charge level is only reported as 75 % (55 % plus 20 %).
To correct the reported charge level, use the "Train Battery" feature. To access this feature, press the [SETUP] key, then the [F1] softkey(labeled "Battery"), then press the [F3] softkey (labeled "Train Battery"), then follow the instructions presented on the screen. This procedure can take overnight to complete.
To keep the reported battery charge level as accurate as possible during extended periods of non-use, the Impulse 6000D/7000DP should be left connected to mains power via the battery charger with the unit powered off in an ambient temperature of 15° C to 26° C (60° F to 78° F). This will continuously trickle-charge the battery (the charge-status LED on the rear panel will be green) to keep both the actual and estimated battery charge level at 100 %.
The ZigBee dongle is a HID, Human Interface Device, and it does not require a driver.
A blinking red charge-status LED indicates a pending charge and should normally last a few seconds before turning solid red. If the blinking continues, the battery-charging circuit has determined that conditions are not correct to initiate the battery-charging cycle. The battery will not be charged if the battery temperature is too cold or too hot. The battery should be charged in an ambient temperature of 10° C to 40° C (50° F to 104° F)
Also, the battery will not be charged if the battery voltage is too low, which can happen if the Impulse 6000/7000DP has been stored for an extended period of time with a fully-discharged battery. In the "Charge Pending" mode, the battery-charging circuit charges the battery at a low rate, which will eventually bring the battery voltage high enough for the normal charge cycle to begin.
No! The SigmaPace1000 is designed to test only one ventricular transcutaneous pacemaker or one transvenous pacemaker at a time. The transvenous pacemaker can be one of these types:
Testing defibrillator energy delivery using internal paddle electrodes, which typically have a curved shape unlike external paddles whose electrodes are flat, is best done using the special internal discharge paddle contacts accessory.
Part Number: 3065438
Description: Internal discharge paddle contacts (set of 2)
Do not use conductive gel when testing internal discharge defibs; the same applies to external discharge adhesive electrodes. The conductive electrolytic gel is only used on patients to improve the contact to the external paddles. The analyzer has very low-resistance contacts that do not require gel.
Clinically, the non-sterile conductive gel is never used inside the patient's thoracic cavity during open heart procedures with the internal discharge paddles. The internal discharge paddle adapters for the Impulse 7000 can be eTO2 gas sterilized and used on sterilized internal discharge paddles, but non-sterile adapters may be used on non-sterilized internal discharge paddles as a pre-test prior to the sterilization process of the paddles.
IMPORTANT These adapters can not be steam sterilized, as it creates too much heat for the plastic parts.
A small amount of drift is acceptable. This type of drift is usually caused by the unit displaying a value that falls in between two digits. Example: You apply 50.5 PSI to the DPM 3, and the reading bounces between 50 psi.and 51 psi. This would be considered normal. If the unit drifts from zero and the displayed readings drift more than one or two counts, the offset my simply need to be zero'ed out, or there may be a problem with the way the DPM 3 is being used, or with the unit itself.
- Fill a syringe (30 mL or so) with distilled water.
- Connect a piece of tubing to the syringe end. Use tubing small enough to be easily inserted into the DPM 3 inlet port.
- Insert tubing ½" or so into the DPM 3 pressure inlet; gently irrigate.
- Empty the syringe into the DPM 3. Hopefully, when the water exits the transducer assembly, the offending debris will be removed with it.
Please contact the Technical Assistance Center if the above suggestions fail to resolve the problem.
The DPM 3 is compatible with all YSI (Yellow Springs Instruments) 700-series temperature probes.
No.
The medTester 5000C can be plugged into a 15-A wall receptacle only when using the 20 A to 15 A power-cord adapter, part number 2195732.
When using the 4-wire method, you are required to null the test lead resistance of your test lead; there is also a slight improvement in test accuracy when the 4-wire method is used. See specifications for detailed comparison.
The 5000C will flash #x.xxx and beep under two conditions when performing power-cord resistance readings. Either the resistance being measured is over 2000 m? or the measurement circuit is not completed. Check to see if the current-source LED light is on. If the light is on, the resistance may be over 2000 m?. If the current-source light is not on, check that you have the Kelvin cable plugged into the two red jacks on the top right of the 5000C, check that the unit under test is plugged into the receptacle on the 5000C, and that the ground pin on the power cord is intact. Then check for an intact ground path. You may need to attach the Kelvin cable to a different location on the case of the unit under test or a grounded lug. When performing a power-cord resistance test you have the option to push SKIP if you do not want to continue with the power cord resistance test. The rest of the safety test will then be completed and your test will not be failed.
No
Typically IP devices have no ground (no protective earth) and no power cord. That means the following cannot be done:
- No protective earth resistance
- No leakage to protective earth
- No single fault tests (there is no power cord---therefore no L1 or L2 wires to open)
That leaves enclosure leakage (touch current).
If the enclosure is plastic (no exposed metal test points) then use a 4 cm square of aluminum foil. This aluminum is taped to the surfaces of the medical device "touchable" by the patient or the clinician who is also touching the patient. Each such available surface must be tested and the maximum leakage reported. The test probe alligator clip is connected to the aluminum foil (which is why it has a certain thickness to prevent tearing), and the measurement is made and compared to the maximum leakage current allowed by the standard. IEC60601-1 and IEC 62353 each have slightly different requirements relative to power on and power off testing.
The medTester 5000C defaults to having the wedge shut off. You can turn the wedge on by pushing the UTIL button, then the right arrow button and then push WEDGE. When you then push ON and STORE your wedge will be turned on. The WPORTS menu in utilities will show you which port on the wedge is to be used by each device. You can change the port used by pushing the up or down arrow buttons and then pushing STORE. Be sure to select the correct baud rate and use the correct cable for your device.
1 ) Printer is not based on PCL5 or ZPLII
2 ) Every time the device and printer are powered off or the printer is connected to another device the printer needs to be reset.
An example procedure to do so:
- ESA615 Reset the printer by:
- "Setup" -> F3 (printer settings) -> F1(Reset Printer)
Explanation: This effect is not an issue when testing actual medical equipment; any current measured through a medical device's CF or BF leads is a result of real leakage through the medical device.
In the situation of one lead only, the Safety Analyzer is measuring the current flow due to its meter capacitance in addition to the current generated by the power source. Any safety analyzer will have some measurable capacitance between Protective Earth and the Analyzer's meter. The design of the Safety Analyzer minimizes this capacitance. When attempting to measure a very low leakage value, such as that from a CF patient monitor lead, even a 20 or 30 µA current can be of concern. However, using a voltage source (mains voltage and resistor) could potentially set up a leakage path from the source coupled through meter's capacitance to Earth. Additionally, switching the polarity of the leads may appear to reduce this problem; in fact, the current is being coupled through capacitance to ground before going through the meter, so less current is detected.
An experiment using an ammeter on either side of the Safety Analyzer will tell you what the "true" current is that flows through the Patient Leads. The amount of current can be different between the ammeter and the Safety Analyzer. The ammeter is a wideband detector, and the Safety Analyzer is designed to replicate a patient's high frequency rolloff based upon the IEC and AAMI standards at approximately 1 kHz, so some higher current is possible on the ammeter if there is a high frequency component to the source.
When evaluating an ESA620, Fluke Biomedical recommends using an isolated power supply as the source: either an isolation transformer powering a calibrator used in the current source mode or an actual AC/DC current source. The best source is a truly isolated source: one that is powered by batteries. If an un-isolated source is used, use a Fluke multimeter on both sides of the Safety Analyzer's connections to determine the "true" current through both patient leads.
Fluke Biomedical has conducted extensive product validation on the ESA620; meter capacitance will not affect the measurements when the Safety Analyzer is used to test medical equipment in accordance with US & International medical device testing standards.
An external keyboard is not needed for the Barcode Scanner to work with the medTester 5000C Wedge accessory. This function may be accomplished by programming the scanner to emulate an external keyboard.
Setting up the medTester 5000C with the Wedge and the Barcode Scanner needs to include the following steps:
- Ensure the Wedge is enabled with the medTester 5000C by selecting UTIL at Menu 1, press the right arrow to go to the second Utilities screen, select Wedge, select ON, and then select Store.
- Ensure the baud rate for COM 1 is at 9600 by selecting UTIL at Menu 1, select Baud, select COM1, press F4 until 9600 is displayed and then Store.
- Plug the Barcode Scanner into the PS/2 port on the side of the Wedge.
- Turn to page 2-6 of the Barcode Scanner User's Guide and scan the Emulate External Keyboard barcode in the middle of the page.
The Barcode Scanner will now scan barcodes and the medTester 5000 keyboard can be used for all other routine user interfaces.
The IEC60601-1:2005 standard now specifies earth leakage limit of 10,000 µA. Test equipment must be capable of measuring results throughout this range for equipment that is in the upper range.
The 454A was designed to protect its relays by not allowing the load to change while the meter is still registering power from the ESU. In other words, the 454A will not change loads until the displayed power reading has dropped to zero. If the power on the ESU was set to 300 W. it can take two or three seconds after you stop firing the ESU before the reading on the 454A will drop to 0 W. During this period of time, if you were to push the CONTINUE button on the 454A and your next step requires a load change on the 454A, the medTester will show the new load value, but the 454A will not switch from the load used on the previous test. As you may have guessed, this could cause your entire test to be failed by the medTester because the next test will be calculated by the 454A using the wrong load. For example, the most often-seen scenario is that you have just completed a monopolar-output test using the 300-? load and your next test is a bipolar output test at 100 ?. The medTester 5000C screen will tell you to set the ESU to fire on bipolar, but the load will still be set to the monopolar 300-? load on the 454A. Your bipolar output test will be calculated using the 300-? load caused a reduced output level and a failure in the medTester autosequence.
No
The ESA 615 is an automated electrical safety that has:
- Built-in automation that allows automatic testing to ANSI/AAMI ES-1 (NFPA-99), IEC62353 (VDE751), IEC60601-1 (2nd, 3rd edition), or AN/NZS 3551.
- Removable memory card with capacity for a minimum of hundreds of test sequences and thousands of test results
- Quick data entry options through plug €˜n' play keyboard, barcode scanner or on-board data entry interface
- Wireless data communication that makes remote operation and data archival fast and simple
- Custom language selections include English, French, German, Spanish, Italian and Portuguese
- An integrated handle that makes the unit easy to carry
To test a monitor with a 5-lead ECG set, use the 10-lead safety test. The fact that you did not attach the additional 5-V leads will not change the test results.
Yes, test sequences can be created and modified per user needs.
The Kelvin cable plugs into the two red jacks on the top left side of the 5000C when taking power-cord resistance or case-leakage readings. If you plug the Kelvin cable into any other jacks, your readings will be incorrect for case leakage, the current source will not be connected for power-cord resistance readings, and you will not get a resistance reading.
ESA615 has the IEC60601 test load that can be selected by choosing this standard in the menu. However, it has the following limitations that do not allow for a fuller compliance with IEC60601:
- For Mains on Applied Part (MAP) testing, source voltage applied is only 100 % of Mains input voltage
- PE test current is 200 mA not 25 A
NO
The ESA615 has built-in test sequences for automatic electrical safety testing. These test sequences provide automatic pass/fail indication to NFPA-99 and other international standards. The unit guides you through the test steps quickly and accurately. Customizable test sequences cover ANSI/AAMI ES-1 (NFPA-99), IEC62353 (VDE751), IEC60601-1 (2nd, 3rd edition), or AN/NZS 3551. The ESA615 does not automate other test devices; however, it can be tethered to other test tools using Ansur automation software.
On Impulse 4000, Main Menu Page 2, there is a MEDT button that needs to be pushed to transfer data back to the medTester. There is also a MEDT selection on the menus of the Impulse 3000 and Dale 900. Make sure that you have pushed this button, that the baud rate is set to 2400, and that you are using the proper cable. The correct cable to use with the Impulse 4000 is Fluke Biomedical part number 2200252. The older part number was 3010-0467. The correct cable to use with the Impulse 3000 and Dale 900 is Fluke Biomedical part number 2199346. The older part number was 3010-0300.
Many SD cards are compatible, but only the 512MB Industrial Grade SD card that ships with ESA615 has been tested and fully validated. Fluke Biomedical strongly encourages you to use the SD card supplied with the instrument. Additional SD cards are available at a minimal cost.
Push CUSTOM on the second menu on the 5000C, then push the right arrow key, and then push INIT. On this menu select SAFETY and make your selections when prompted. Remember these selections will be changed on all of the safety tests.
The IEC60601-1:2005 standard refers to patient and patient auxiliary leakage readings in both AC and DC parameters. If a safety analyzer only displays True RMS, you are not documenting all the results needed.
No
Make sure that you are using COMM 2 on the medtester. The correct cable to use is Fluke part number 2200252. The older part number was 3010-0467. The baud rates on both COMM 2 of the Medtester and the Impulse 4000 need to be set at 2400 baud for the connection to be successful. When you use the defib module on the 5000C the baud rate should automatically change from any baud rate to 2400 baud by itself. Therefore whatever the baud rate was set at for COMM 2 you will still get a connection. This is not true when using the pacer module on the medtester. You will need to physically change the baud rate to 2400 baud in the UTIL menu under BAUD. Make sure that the Impulse 4000 is on Main Menu Page 1 when you start the autosequence in the medtester.
The ESA615 will attempt to load the last test sequence used on power up. If you have deleted it, for instance by reimaging your card, you will need to select a test sequences from the test library. Push F4 to say "OK" and then push F3 for "Test Library" and either select a test sequence or create a new one to resolve this error.
A Kelvin cable is a coiled cable with a double banana-plug connector on one end and a clamp on the other end. This can be ordered from Fluke Biomedical, part number 2392617
No. The ESA615 does not have the ability to use a 4-wire method to measure earth conductor integrity. If this method is required, we recommend the ESA620.
1. Change the type of tester by pushing the right arrow key so that you are on Menu 2 on the medtester. Now push the CUSTOM button and then AUTOSEQ. Push the IVPUMP button and then push TYPE. Now you can select INFUTEST and then push STORE.
2. You must now initialize the medtester autosequences for the test. To do this push the CUSTOM button on Menu 2 and then push INIT. Now push IVPUMP and then push YES.
3. Check the baud rate on comm. 2 to make sure that it is on the correct baud rate for your tester. You are now ready to test using the correct tester. The same sequence can be used for changing the type of SPO2 tester that you use with your medtester.
The following test sequences are included with the ESA615:
- IEC60601-1 3rd Edition: Patient Monitor, Defibrillator, Infusion Pump, Ultrasound Device, Generic Device and System
- IEC62353: Patient Monitor, Defibrillator, Infusion Pump, Ultrasound Device and Generic Device
- NFPA-99 (Hospital): Patient Monitor, Defibrillator, Infusion Pump, Ultrasound Device and Generic Device
- ANSI/AAMI ES1: Patient Monitor, Defibrillator, Infusion Pump, Ultrasound
No
On Impulse 4000 Main Menu Page 2 there is a MEDT button that needs to be pushed to transfer data back to the medtester. Make sure that you have entered the baud rate at 2400 and that you are using the proper cable. The correct cable to use is Fluke part number 2200252. The older part number was 3010-0467.
Be careful not to run automated tests from old firmware versions. You need to recreate any custom test sequences after updating to the latest firmware to receive all the benefits from the update.
- Avoid using Windows ReadyBoost. It will cause problems when the SD card is installed in an ESA615.
Module 5 is called the Waveforms/Extended Testing module. Module 5 gives your medTester 5000C some useful testing abilities plus ECG, arrhythmia and performance waveforms. Without Module 5, a 5000C has ten built-in safety tests. With Module 5 installed in your 5000C, you will get an additional five blank safety tests that can be programmed to perform the exact safety test steps that you need to do without changing the integrity of the ten base safety tests. There are two additional tests which can be very helpful to you. The line monitor test will monitor the line voltage supplied to the receptacle that the 5000C is plugged into and record changes in voltage over extended periods of time. The environmental monitor allows you to record both ground potential voltage and resistance measurements between a common ground point and up to 99 other ground points.
Do not double-click an ESA612 Data Viewer .CSV file to open it in Excel if your computer is configured for a regional setting that does not match the US settings. You can configure the settings to match your regional setting as follows:
- Rename the .CSV file to a .TXT file
- Start Excel
- Choose File/Open and set "Files of type" to All Files (*.*)
- Select the desired .TXT file and press Open
- On the first screen that appears you select "Delimited":
- On the second screen you select "Comma":
- On the next screen you click the "Advanced" button and change the Decimal separator to period "."
- Click the Finish button and the file will be imported.
Yes, except the limitations mentioned above (MAP source voltage 100 % of mains input and PE test current of 200 mA), the ESA615 tests according to IEC60601 2nd and 3rd editions.
Although safety analyzers normally display the test results in µA, this is not true when using it with a 202A LIM tester. The 5000C display now is reading in mA so there is no need to convert the reading. The medtester 5000C needs to be in the MANUAL ISOPWR test mode for use with a 202A LIM tester. The double banana connector on the 202A needs to be plugged into the 5000C correctly. If you look at the banana plug you will see that this cable has one connector on the double banana connector that has a tab with the letters GND stamped on it. This ground side of the double banana connector should be plugged into the black external input jack while the other side plugs into the red external input jack.
This is a limitation of the file system on the SD card (FAT16/FAT32). You can avoid this behavior by naming your test with more than 8 characters.
No
No. If you plug a piece of equipment into the receptacle on a 5000C that has only two conductors, you will get no resistance or leakage measurements because there is no ground conductor. Power cord resistance and leakage measurements are taken through the ground wire.
- Put the SD card into any USB memory card reader (not included).
- Save any test results (.DTA) files you wish to retain.
- Download the latest ESA615 Firmware Update from www.flukebiomedical.com under Support > Software Downloads.
- Verify your ESA615 firmware is up to date (look for it on power up or under Setup > Instrument Information). Update your firmware using the firmware update instructions, if needed.
- With the SD card installed on a Windows PC, follow the firmware update instructions to "Update SD card with new factory image". For firmware version 2.05, it is steps 13 to 25 in the firmware update instructions.
Under the safety-test selections there are two different types of safety tests: external leakage tests and internal leakage tests. The external leakage tests are used to test case-surface leakage. Since you are testing for leakage on the surface of the unit, you must first connect the Kelvin cable to the metal surface or a grounded lug on the unit under test. The other set of test positions are the internal-leakage tests. These tests will measure leakage that is on the ground wire inside of the power cord. The Kelvin cable does not need to be attached for this test.
All electrical safety plug-ins power off, then apply a delay to ensure a minimum time with power turned off before turning it on again, in addition to letting the device under test (DUT) stabilize after powering off.
This is also consistent with the way the Power On Delay is implemented. The DUT power is switched on and then the delay is applied, allowing the DUT to stabilize after powering on.
If you want to perform any actions before powering a DUT on or off , you should use the "Stop before new power configuration" and/or "stop after new power configuration" options.
Yes, it has a power supply that can accept both 120 V and 220 V; however the test receptacle is configured for one or the other.
The newer medtester 5000Cs have a Clock Enable Switch on the right side of the 5000C. Go to the UTIL menu and push the CLOCK button. After you change the time and date, push a non-metallic probe through the lower right vent hole on the right side of the 5000C and push in the micro switch lever. Hold this lever in while pushing the STORE button on the menu. Now you can release both the switch and the STORE button. When you escape to the first menu, the clock should be running and the time and date should be correctly set.
Yes, test results can be printed by a serial printer (Such as the DPU-414, P/N 2248899) which is connected to the RF303RS serial port.
- Put your RF303RS into "simplex" mode. To do this:
- With the RF303RSturned off, hold down the "+" and "-" softkeys (used to select load resistance)
- With the "+" and "-" soft keys depressed, turn on the RF303RS. Wait a moment, then release the soft keys
- Your RF303RS is now in simplex mode. Using a straight-through serial cable, connect your printer to the RF303RS serial port. The RF303RS serial port is configured as follows: Baud rate is fixed at 2400. No parity, 1 stop bit. Configure your printer to the same settings the RF303RS uses, as shown above.
- Turn on your printer. Put it "on line".
- Take a power measurement reading. While the reading is being taken, push the "mode" button.
- Data will be sent to your printer showing power in watts and current, as well as load resistance. Carriage Return and Line-feed signals will be sent to your printer.
- Every time you push the "mode" button, one line of data will be sent to your printer.
No. Microsoft Excel requires a comma-delimited file. Output from the RF303RS is formatted to be displayed properly by your printer, or on your computer monitor. RF303RS data is not comma-delimited.
- Interpreting RF303RS Fluctuating Readings
- The model RF303RS incorporates an accurate digital measuring system that has three modes. The first measurement mode (default mode) utilizes a relatively short sampling time and does not filter or average ESU output. The two selectable measurement modes utilize longer sampling times that tend to average ESU output. When using the default measurement mode, you may observe some electrosurgery units (ESU) output readings that fluctuate plus or minus 10% or more depending on the unit under test. This is normal operation and is not indicative of a problem with the RF303RS.
- Determining if the ESU is the Problem
- When fluctuating readings are observed with the RF303RS, the technician should take note and determine if this is normal behavior for the ESU under test, or if this behavior is a sign of a problem.
- It May be Normal
- If a fluctuating output is normal for a particular ESU (as determined by the manufacturer, see accuracy specifications for ESU), the user can calculate the average of the high and low reading observed on the RF303RS (fluctuating readings may be discernable on the RF303 display) or the user can utilize the RF303RS's Signal Averaging Mode (SAM).
- Older ESUs may have unstable output due to old technology or design. This is typical and is acceptable based on the manufacturer's limits.
- Many newer-generation ESUs utilize instantaneous feedback loops, which constantly adjust the output and can cause an oscillating effect. This is also satisfactory and is considered normal for these devices.
- It May be Broken
- In some cases, fluctuating ESU power output is evidence of a problem. Fluctuating output on some ESUs may indicate the weakening of output from power transistors or other ESU ailments and is not acceptable.
- Signal Averaging Measurement (SAM)
- If an ESU normally has fluctuating output, then operating the RF303RS in one of its Signal Averaging Measurement (SAM) modes makes sense. SAM significantly reduces fluctuating readings on the display of the RF303RS making it easy for the technician to read an average value.
- Upon power up the RF303RS defaults to the instantaneous algorithm for power output measurement which shows fluctuating ESU output. The user can select SAM by depressing the "mode select" and "- ohm select" keys simultaneously; each time the user initiates this key sequence the RF303RS will increment to the next mode, displaying "F X" momentarily. Starting at the default mode ("F 0"), the first mode entered is the one second sampling mode, ("F 1"); initiating the key sequence again will select the two second sampling mode ("F 2"), initiating the key sequence again brings the unit back to the default instantaneous mode and so on.
- Bottom Line
- If you observe fluctuating power readings on the RF303RS, it is likely that the ESU being tested has a fluctuating output signal. To obtain an average power reading, select the RF303RS's signal averaging mode.
The load resistors typically used in ESU analyzers are not "ideal". They possess some reactive components that are frequency dependent. The RF303RS derives applied power by measuring the voltage across the set load and calculating the power (V2/R). Most other ESU analyzers on the market derive the applied power by measuring the current flowing through a set load and calculating the power (I2*R). At fundamental frequencies below 500 kHz and regardless of the load setting, the two methods of measurement are comparable. Above 500 kHz, and at the extremes of the loads, the readings displayed by the two methods will differ on opposite sides of the expected value.
As an example, when testing the Conmed Excalibur Electrosurgical Unit in the monopolar output with the RF303RS load set to 50 ?, the set value on the Conmed will correlate with the displayed value on the RF303. When in the Bipolar mode, the RF303RS will display higher than expected values - up to 35% higher. The same test performed on some current measuring analyzers will produce lower than expected values. This is due to the difference in fundamental frequencies between the monopolar and bipolar modes. In this case, the Conmed operates at 500 kHz in monopolar mode and 1 MHz in bipolar mode. When comparing readings measured with a V2/R device to readings measured with an I2*R device, total measurement difference will likely be larger than 35%, due to different methods of deriving power.
This does not mean that the RF303RS is malfunctioning or in error. Rather, it reflects the different results the two measurement techniques will produce when the load deviates from the nominal value used in the power calculations. It should be noted that most ESU manufacturers use the current measuring technique to calibrate production units.
This characteristic does not affect Electrosurgical Units that operate with a fundamental frequency less than 500 kHz, such as ValleyLab electrosurgical units.
Firmware is field-upgradeable and downloadable from our site at the gas flow software page. The link will state whether a calibration is required. Your device will always be upgraded to the most recent firmware version if your device is sent to a Fluke service center.
The connection to our gas flow analyzers changes depending on the testing you are about to do.
If you are testing breath parameters or bi-directional flow the connection should be a Y connector on the flow inlet side and a calibrated test lung on the flow exhaust side. Always use an antibacterial filter on the inlet side to elongate the life and accuracy of your gas flow analyzer.
When testing uni-directional flow or concentration measurements the DUT simply needs to be connected to the flow inlet side using an antibacterial filter.
All of these products have an 8-hour battery life allowing you to test all day, on-the-go.
The features that differentiate the VT900A and VT650 are the ability to measure ultra-low flow and ultra-low pressure, the ability to use an external TTL trigger input and improved oxygen sensor accuracy and lifetime (1% accuracy and a 2-year lifetime vs. 2% accuracy and a 1-year lifetime).
Saving results is easy on any of these units. From any screen there is a blue box in the bottom right called “Save”. Press on this button and you are able to save your results as data, a graph, a recording or under a new Test ID. These results can then be recalled from the onboard memory under “Menus” and “Memory”.
From a technical standpoint, there is no difference between the VT900 and the VT900A. The only difference is that a connector was added at the rear panel to allow for power and communication to the VAPOR Anesthesia Tester.
Under “Menus” and “Special Tests” there are a number of tests that can help troubleshoot and identify failure modes. These tests include:
- Airway Pressure Leak Test
- High Pressure Leak Test
- Low Pressure Leak Test
- Ultra-Low Pressure Leak Test
- Trend Test
- Stacked Volume Test
- High Frequency Test
There are two sensors to zero on these devices. The first is the airway flow sensor. You want to zero this without the breathing circuit attached. From the “Airway” screen, press “Zero”.
The second sensor to calibrate is the oxygen sensor. From the “Menus” screen, press “Calibrate Oxygen” and the device will lead you through the steps to calibrate your sensor using air and oxygen.
By upgrading to VT PLUS HF. Any VT PLUS can be upgraded to allow full RT-200 capability. VT PLUS HF responds to the full RT-200 command set when you select the RT-200 emulation mode. It's as simple as entering the RT-200 function key number and then the BACK button on the VT PLUS HF RT-200 emulation menu.
The VAPOR Anesthesia Tester is an accessory to the VT900A that allows for preventive maintenance / efficacy testing of vaporizers. VAPOR can test the concentration of 5 major anesthetic agents, CO2 and N2O.
There are certain applications that require high resolution and high accuracy to ensure functional performance. Examples of such devices would be anesthesia machines and neonatal ventilators. In these applications, you simply connect the tubing to the ports on the nearside of the VT900A and switch your screen to the ultra-low flow and ultra-low pressure views.
The connection to our gas flow analyzers changes depending on the testing you are about to do.
If you are testing breath parameters or bi-directional flow the connection should be a Y connector on the flow inlet side and a calibrated test lung on the flow exhaust side. Always use an antibacterial filter on the inlet side to elongate the life and accuracy of your gas flow analyzer.
When testing uni-directional flow or concentration measurements the DUT simply needs to be connected to the flow inlet side using an antibacterial filter.
If you have HFOV units in your ventilator fleet, their performance must be evaluated to ensure that it meets the manufacturer's specifications. VT PLUS HF helps you quickly make the evaluation by simply connecting to the patient Y of the ventilator breathing circuit, making one or a series of measurements, and comparing them to the HFOV control settings and manufacturer's specification tolerances. You can document all this by printing out the graphical and numeric display of data from VT PLUS HF and filing it with your other test data.
VT900 lacks the connector on the rear panel that provides power and communication to the VAPOR Anesthesia Tester. Only the VT900A has this connector.
The Excel Plug-In is used to download test data to your PC for upload. The Excel Plug-In can download numerical data as well as graphs to ensure that you are able to get your test results into a report and even into your CMMS. Easily download the Plug-In from the gas flow analyzer software page and install on your PC.
The connection of VT900A for testing the ventilator function of an anesthesia delivery system is unchanged from normal breath by breath or constant flow testing.
VAPOR needs to be used to test the anesthetic agent concentrations as well as carrier gas concentrations. VAPOR is connected to the VT900A using the connector on the back of the VT900A. The inlet should be connected to the fresh gas outlet using a tee connector to pull a side stream sample. The exhaust ends of the tee connector and VAPOR should be connected to the anesthesia gas scavenging system (AGSS).
WARNINGS:
- Do not run anesthetic agent through any ports of the VT900A.
- Only pull side stream samples into VAPOR using a tee accessory.
Firmware is field-upgradeable and downloadable from our site at the gas flow software page. The link will state whether a calibration is required. Your device will always be upgraded to the most recent firmware version if your device is sent to a Fluke service center.
The COVID 19 virus particle size is 125 nanometers (0.125 microns); the range is 0.06 microns to .14 microns. The bacteria filter shipped in the accessory kit for VT gas flow analyzers filters down to 0.3 microns. It is not designed to stop COVID-19, but it is designed to protect the flow and pressure sensors of the VT gas flow analyzers and should be use during all medical gas flow/pressure measurements when using the main flow channel. Using a filter helps extend the life of your analyzer and the accuracy of your results by keeping your channels and sensors clean.
The breath detection mode should be changed depending on what it is that you are testing. Breath detection modes can be changed under “Menus”, “Setup”, “Breath Detect”.
If you are testing breath parameters using a test lung, you want to be in bi-directional mode. This will allow the flows to pass through the gas flow analyzer in both directions to simulate human breathing.
Uni-directional flow or continuous “off” flow is used when testing parameters that should be at a constant setting (flow rates, oxygen concentration). This allows for the gases to pass through the gas flow analyzer in only one direction.
Start the first channel.
Select STATUS to return to the "Status All Channels" screen.
Select the next channel you want to start.
Follow the same start procedure for each channel.
The RS232 ports (Serial Port) on your computer and IDA 4 Plus must be configured the same way. Hydrograph for Windows assumes the IDA 4 Plus RS232 port to be set to its default: 19,200 baud.
Verify that your IDA 4 Plus RS232 port is set to 19,200 baud. RS232 settings be viewed in the Utilities menu.
If using Hydrograph for Windows, verify that Hydrograph has configured your RS232 port to 19,200 baud. In Hydrograph, RS232 port settings can be viewed and changed, by clicking "Control" on the menu bar, then by selecting the "Com Port Settings" option.
If your computer has more than one RS232 port, follow the directions shown above to verify that you have selected the RS232 port used to connect your IDA 4 Plus to your PC.
Verify that the correct serial cable (P/N 2392046) is being used.
There are a number of USB-to-Serial adapters that can be connected to the IDA 4 Plus for communication. We recommend the Digi Edgeport/1 (DB-9) adapter for use with the IDA 4 Plus.
The IDA 4 Plus computes flow rate by measuring the time it takes to fill a glass tube of known volume. The IDA 4 Plus senses when the measuring tube is filled, then drains the measuring tube, and the cycle begins again. While the measuring tube is being drained, the IDA 4 Plus occludes its inlet. This is the clicking sound the IDA 4 Plus makes.
The measuring tube used by the IDA 4 Plus is about 1 mL. When testing flow at high flow rates, (over 800 mL/hr, for example), the measuring tube fills very quickly, and must be drained more frequently. Your infusion pump may be sensing the brief (but more frequent) occlusion of the IDA 4 Plus inlet.
Suggestions:
- Increase the length of tubing connecting your infusion pump and the IDA 4 Plus inlet. This may act to "cushion" the effect of the occlusion of the IDA 4 Plus inlet.
- Check that your tubing has no kinks or sharp bends, and that the tubing interior diameter is at least 1/8".
- Check that the drain receptacle is placed lower than the IDA 4 Plus.
- If the above steps fail, try testing a different (same model) infusion pump. If the problem persists, it may be necessary to test at a lower flow rate.
The syringe must be filled with water, not saline or any other liquid. Inspect the water in the syringe, purge out any air before priming.
Add a single drop (per 100 mL) of dishwashing detergent (Dawn works well) to your water. The detergent is not used as a cleanser, it is used to make the water "slippery", this helps prevent drops that cling to the IDA 4 Plus internal measuring tube.
When priming, infuse steadily and slowly. This won't slow you down, priming only takes a moment.
Your IDA 4 Plus requires Firmware Version 2.10 to work properly with Hydrograph for Windows, Version 2.05. The required firmware was included with Hydrograph for Windows, Version 2.05, along with installation instructions.
Hydrograph for Windows attempts to connect with your IDA 4 Plus when it is launched. Your IDA 4 Plus should be turned on and connected to your computer before Hydrograph is started.
If Hydrograph failed to connect for this reason, you can force Hydrograph to connect with your IDA 4 Plus by clicking the "Control" option on the menu bar, then scrolling down to, and clicking on "Connect".
It is very important to clear all air bubbles from the infusion set tubing and the priming syringe and stop-cocks before any testing begins. Sometimes, even when this has been done, an air bubble will form inside the measurement system of the IDA4. This bubble may not affect anything until the internal burette empties and the bubble is sensed by the optical sensors, causing the error described. Such bubbles must be cleared in order to continue.
To clear internal bubbles, disconnect the infusion set tubing, stop-cock, and priming syringe from the IDA4 PLUS channel fitting. Fill a syringe with water which has been treated as prescribed in the IDA4 Operators manual, and flush the IDA4 PLUS measurement channel via the affected channel's input fitting. This may need to be repeated to clear pesky bubbles. Reconnect the infusion set tubing, stop-cock, and priming syringe being careful not to introduce a new bubble in the process. Repeat the measurement.
In order to use the Wedge Adapter, a specific cable must be used to allow the medTester to communicate with the IDA 4 Plus. This cable can be ordered from Fluke Biomedical, part number 2201042.
To run Hydrograph for Windows on Windows 98/2000/XT, Hydrograph for Windows Version 2.05 is required.
It is very important that no air is present in the pump, bag, syringe or tubing.
Add a single drop (per 100 mL) of dishwashing detergent (Dawn works well) to your water. The detergent is not used as a cleanser, it is used to make the water "slippery". This helps prevent drops that cling to the IDA 4 Plus internal measuring tube.
Use only water. Use of saline or any liquid other than water is not recommended. Use of a liquid other than water can dirty the IDA 4 Plus internal glassware, resulting in poor priming, error messages, or loss of accuracy.
Yes, Test Groups will complete automatically. HOWEVER, before you create a test group, it is highly recommended that you go through each test and understand what the test will require from you (the user). For example, if a test group is created and includes the Inside Alarm level, the device will not automatically carry out the test; you need to be there to manually turn on the alarm to get a reading for the test. Another example is airflow; to measure airflow properly, a reading must be taken from the center and each quadrant thus requiring the airflow probe to be moved about the environment. This means that with certain tests, the device cannot be simply placed into the test environment and left alone for several hours; interaction is needed with both the device and DUT for the INCU II to complete the test and continue through the Test Group. Read through the tests beforehand to ensure you understand what is required from you as the user to avoid this.
A great solution is to create two test groups one with all the tests you need to perform that require your interaction with the device, and the other with the tests that are hands-free and allow you to perform other activities while it is testing. It might be beneficial to group all temperature tests into one Test Group, to avoid disturbing the test environment as much as possible.
No. The INCU is designed to collect data from one incubator at a time. At the completion of each incubator test, the data can be uploaded to the PC using the INCU PC software, and can then be archived to storage media (hard drive, external drive, CD ROM, etc).
The temperature probes are for closed-environment testing, so are to be used in incubators and transport incubators. The temperature pucks are specifically for radiant warmers. If the temperature probes were used in a radiant warmer, the readings would not be accurate; a vent, breeze, or any air movement would severely affect the temperature readings. The temperature pucks are designed to absorb the heat given from the radiant warmer, so external air movement will not affect their reading.
INCU II has a mini Ansur plug-in not a full Ansur plug in. The mini Ansur plug-in is what provides the interaction between your personal computer and the INCU II device to allow test results to be transferred to your computer. The INCU II does NOT have full Ansur compatibility, but the "Create a Test Group" option and Excel Add-In allow you to standardize your workflow and create a report specific to your needs.
Although the INCU PC software wasn't originally designed to export data directly to EXCEL, this option does exist. The INCU Operator's Manual, Appendix C, contains the data file format for exporting INCU data to a database. Converting the saved INCU data file to a semicolon delimited file will help in importing the data into EXCEL. The process may take several steps.
INCU data format:
- All the data must be divided by 10 except for air-flow data
- Air flow data must be divided by 100.
- The character "M" preceding the value indicates an event marker. This character must be suppressed from the all data to obtain a numeric value.
After the initial "stabilizing" period of the airflow probe, the INCU II will then display the airflow measurement. If the airflow inside the test environment is at or over 2.1 m/sec, the INCU II will display "OL", meaning the airflow is above the outer limit. Keep in mind that according to IEC 60601-2-19, 2-20, and 2-21 standards, an acceptable airflow measurement is at or below 0.35 m/sec.
No. The placement pad is merely a guide to help you correctly place the INCU II device in the center and probes in the center of the four quadrants of the mattress. The pad is an average mattress size, so if the mattress of the incubator/radiant warmer in your facility is not the exact size, the pad will not tell you EXACTLY where the center is but it serves as a guide. There are detailed instructions in the User's Manual to find the center and center of each quadrant, but you will find that the placement pad is helpful and intuitive to use.
The INCU uses a hot-wire anemometer to measure air flow within the incubator. Since heat and enriched oxygen environments don't mix due to increased potential for flammability, evaluating the oxygen concentration should be done separately from the rest of the testing. Fluke Biomedical offers the max02 PLUS AE Oxygen Monitor, ideal for this type of analysis.
To learn more, register and/or visit our Advantage Training website at: Advantage Training
If wireless is available in your country, you can upgrade your INCU II device from non-wireless to wireless with a simple numeric code entered into the "Wireless Configuration" option in the "SETUP" menu. To get this number, contact Order Management or Service with your unit's serial number, and they will generate the numeric code for you. Ask your local representative if wireless if available in your country, and to find out more.
The laws of thermal dynamics come into play, as well as the need to evaluate the temperature-control circuit operations sufficiently. It takes time for the incubator chamber to warm up (equilibrate) to the temperature control value set on the incubator controls. Once the chamber is at a uniform temperature (as evaluated by the four separate, but simultaneous, thermistor measurements), the temperature control-circuit operation can best be evaluated. It would be expected that the temperature be controlled within the accuracy band provided in the incubator manufacturer's specifications. This should also agree with the IEC Standard requirements. Shorter test durations may not catch faulty temperature control circuitry.
There are two models available: Non-wireless (4722635) and Wireless (4722620). Wireless is not available in all countries, and some customers specifically request non-wireless for their facility, so a non-wireless version was made available. Although a non-wireless unit can be upgraded to a wireless version if desired and permitted in your country, wireless cannot be "turned off" once it is activated. Thus the need for two different models.
The placement pad is a microfiber cloth it is not antimicrobial. Whenever an incubator or radiant warmer is tested or serviced, it should be thoroughly cleaned and sanitized before being used by a patient again, so sanitizing the placement pad or INCU II device before or after each use is not necessary.
The INCU II requires calibration every 12 months (once per year). The INCU II should be returned to a Fluke Biomedical authorized service center under an RMA (Return Materials Authorization) with all its sensors. When a unit is returned, we verify that all supplied probes and pucks are performing within specifications along with the INCU II unit itself.
When airflow is being measured by the INCU II, the probe will need to detect a steady airflow before it begins its measurement "stabilizing". Once it has done so, it will record the measurements and display them in real-time on the device. The "OL" signifies that the measurement is beyond the specified range of the INCU II Analyzer, meaning that the airflow being measured is above 2.10 m/s. If the airflow is below 0.10 m/s, the unit will display "0.10 m/s."
To maximize accurate airflow measurements, position the airflow probe perpendicular to the air flow in the DUT and without any obstructions to interfere with the airflow path to the probe. Refer to the User's Manual for more a more detailed description.
The pucks were designed specifically to the IEC 60601-2-21 standards for Radiant Warmer testing. The standard calls for the material, circumference, mass, and density of the pucks. The pucks are made of aluminum, which allow them to absorb heat from the radiant warmer.
Because the pucks add quite a bit of additional weight, and we realize that incubators and radiant warmers may not be tested at the same time, we have created a separate carrying case for the pucks.
The General Testing option will allow you to log data in real-time for all probes plugged in for however long you choose (refer to question #6). The Standards-based Tests ("Choose an Environment") contain lists of tests that are specific to the IEC standard for the environment in which you are testing. When you have finished your General Test, you will need to perform your own test analysis for the results that are achieved to understand whether or not a test has passed or failed to your own protocols. The Standards-based Tests will show Pass/Fail indicators at the end of each test for easy test analysis, and you can also create Test Groups with this feature for automated test completion.
If a probe is found out of spec, we replace the probe/puck with a new probe/puck and perform verification again.
NO. You will notice that each probe has a tag on its wire with numbers these are that probe's calibration numbers. Each probe is specifically calibrated to its respective port which is why the probes are labelled and color-coded. Although the temperature probes/pucks will fit into the other ports and even take a reading, if they are not plugged in into the correct ports, the reading will not be accurate. It is critical that the probes/pucks are plugged into their respective labelled/color-coded ports.
Because each probe is specifically calibrated to its port, probes (temperature and every other parameter) cannot be interchanged between devices unless both devices are calibrated with that probe's calibration numbers.
If you need to replace a probe, you will have to enter in its calibration numbers into the respective probe in "Probe Information" in the "SETUP" menu.
The IEC standards reflect the best experience of the industry, researchers, consumers, and regulators worldwide. The standards help establish a universal and uniform testing procedure for biomedical/clinical, service, and design engineers to use, and are critical in helping properly assess the safety of medical devices and ensuring patient safety¹. The procedures called out in the testing/service manuals of many medical device manufacturers are often built around these standards. The INCU II was specifically designed around the IEC 60601-2-19 (incubator), 2-20 (transport incubator) and 2-21 (radiant warmer) testing standards.
Minimize risk, maximize patient safety. Test to the standards. To learn more about the standards, visit http://www.iec.ch/about/activities/standards.htm¹
No.
The General Testing option is a highlighted feature of the INCU II. The General Test option is basically a data-logging mode; any probe that is plugged in be it a temperature probe(s), pucks, airflow, sound, humidity, etc. and every combination thereof the INCU II will take continuous measurements until you stop the test. With this option, you can complete a test in 15 minutes (after STC has been achieved) or up to 48 hours.
The General Test gives you the freedom to do perform non-standards based testing that is specific to your facility; you can create a unique protocol specific to your needs. Another great example of using the General Testing is to do a "quick test" of the incubator/radiant warmer after it has been serviced, to ensure all parameters are within range in a quick manner.
It is possible to replace a probe in the field; however, to know if it is performing within specification, it must be verified against a known reference standard – this is what we do at the Fluke Biomedical Authorized Service Center. To ensure a fully calibrated unit, a customer must send the mainframe and all probes in for calibration.
There are two different types of sequential procedures that can be used in the medSim 300B menu. The first is called auto sequences. These are eight preprogrammed sequences that run by automatically without showing the current simulation on the screen of the medSim 300B and no user interaction. The second type of sequential procedure is the step sequences. These can be started and stopped by the user prompts on the screen of the medSim 300B. There are three preprogrammed step sequences which include CCU, Holter and Pacemaker series. The other four step sequences are User sequences which can be completely programmed by the user to include several different types of simulations. You can program up to 20 simulation segments that will each run from 0.0 to 99 minutes. Each of these segments can be started and stopped at any time by the user.
The more IBP channels a simulator has, the larger and more expensive the simulator will be. The majority of our fleet of customer design partners reported they do not have to use more than two IBP channels at the same time; those who do need to test three or more IBP channels have chosen to test two IBP channels at a time, then two more, and so on. This preference avoids that extra cost, size and weight, and still yields faster/easier testing in the end.
Alternatively, the new ProSim 3 does have four IBP channels thatyou can test all simultaneously.
No, when you use the SHIFT function in the CuffLink you are moving the entire pressure envelope waveform thereby changing both the systolic and diastolic pressures at the same time. You can not change just one of the pressures.
ProSim 4 and 8 batteries must be charged using the model-specific battery eliminator shipped with each device. For this reason Fluke Biomedical has:
- Made clear mention of it in the user manuals.
- Added a colored flag to the battery charger (ProSim 4 = yellow label, ProSim 8 = red label).
- Designed electrical protection from possible burn-out from application of the wrong battery charger. Please keep in mind: though this protection is in place, using the wrong battery charger can cause loss of some battery life if connected to the wrong voltage for extended periods of time.
Masimo Rainbow is the first technology to noninvasively measure blood constituents and fluid responsiveness that previously required invasive procedures. Besides measuring arterial oxygen-saturation level (SpO2) and pulse rate, Rainbow technology measures following parameters as well: Hemoglobin (SpHb), Carboxyhemoglobin (SpCO) and Methemoglobin (SpMet).
Traditional Pulse oximeters use wavelengths of two lights (infrared light at 940 nm and red light at 660 nm), which are absorbed differently by either oxyhemoglobin or the reduced hemoglobin to measure SpO2 concentration. Two-wavelength oximeters cannot measure total hemoglobin or dyshemoglobins. Rainbow sensor technology uses more than 7 wavelengths of light to acquire blood constituent data based on light absorption.
Check to make sure that the ends of the coiled cable are plugged into the controller and the Keypad jack on the DataSim 6100. If both ends are correctly plugged into the controller and the DataSim 6100, and something other than NSR is seen on the controller screen or if the screen is blank. Check to see if the power light is on. If not, try charging the unit. If the power light is on and you see something other than NSR on the controller display, send the DataSim in for repair.
Reflectance type probes are not compatible with Index 2 series simulators.
Blood pressure can be measured using a variety of techniques, which can be classified into two major categories: invasive and non-invasive. The invasive approach inserts a catheter into an artery of a test subject. The catheter may contain a pressure transducer at its tip or it may be fluid-filled and couple the blood pressure through the fluid to an external transducer. The change of fluid pressure (blood pressure) in the subject's artery is measured invasively. This technique is also referred to as a direct measurement, because the parameter being measured is directly coupled to the transducer. Non-invasive blood pressure measurement usually involves the use of an inflatable cuff wrapped around the limb of a test subject. The cuff is inflated and deflated at a controlled rate and physical parameters are observed. The auscultatory and oscillometric techniques are well known non-invasive methods. These methods are indirect because they do not couple directly to the artery. ProSim 8 and 4 simulates oscillmetric technique since modern NIBP monitors now use oscillometric technique to measure pressure.
Two cables are needed to do temperature simulations on these monitors. These two cables plug into each other to become the temperature line from the medSim 300B to the temperature module. The two cables that you will need are the HP temperature adapter, part number 2199257, and the YSI 400 series temperature cable, part number 2523334.
Alarm hazards ranks second on the Heath Technology Hazards of 2011. The Boston Globe recently reported the death of a patient whose treatment have been delayed because a critical physiologic monitoring alarm had been turned off.
There are both static and dynamic simulations that can be sent from the CuffLink. Accuracy specifications refer to static blood pressure measurements such as the "Manometer" test. The static pressure tests are normally very accurate. Since the usual test function of the CuffLink is to provide a dynamic blood pressure simulation such as 120/80, and due to the probable difference between the algorithm used by the CuffLink and the algorithm expected by the monitor, perfect accuracy can not be expected. The simulation that you select on the CuffLink may vary from the reading displayed by the monitor. Repeatability is much more important. Every time that you use the CuffLink to simulate a given pressure with each type of monitor, the readings should be very close to being the same as the last test on that type of monitor.
70 % of the original capacity with operation at 25 °C room temperature.
If your medSim 300B has the cardiac output option installed CO will be in the F1 position on the second menu of your medSim 300B. If cardiac output is not installed the F1 position will be blank. Your medSim 300B can be upgraded to give you the cardiac output option.
No. Ensure both ProSim 4 or 8 and patient monitor are properly zeroed before starting the IBP simulation. Below is the step by step procedure on how to properly zero both patient monitor and ProSim 8 for IBP number to display. Please the zero procedure on different patient monitors may be different; please refer to patient monitor user manual for details. The example below uses HP/Philips Viridia vital sign patient monitor:
- Connect ProSim 8 and HP Viridia monitor with proper IBP cables
- Select IBP on ProSim 8, ZERO both IBP channels
- On HP/Viridia, select MODULE SETUP
- Then select PRESS 1 ABP
- Press ZERO XDUCER
- ZERO IN PROCESS should display on the monitor
- Initiate the ProSim 8 IBP simulation. IBP numbers should display on the HP Viridia monitor
No, the CuffLink can simulate neonate and adult blood pressures but not wrist cuff pressures.
For optimum shelf life in consideration of practicality, we suggest keeping the battery at 30 % to 50 % state-of-charge. There is a non-recoverable capacity loss upon aging. The higher the state of charge & temperature, the higher the percentage of non-recoverable capacity lost. We estimate a 100 % state-of-charge under 25 °C room temperature will have about 15 % capacity loss per year of storage.
Yes.
Ventricular Fibrillation (VFIB) is a medical emergency condition in which there is uncoordinated contraction of the cardiac muscle of the ventricles in the heart, making them tremble rather than contract properly. Since the VFIB waveform continuously changes in shape, magnitude and direction, different patient monitors may use slightly different algorithms to detect VFIB signal.
When running the PS410/420's electronically-generated VFIB selection on either the SpaceLabs Healthcare UltraView 1500 or the Datascope Corporation Passport 2 patient monitors, the signal is not always recognized as VFIB. Randomly, short waveform segments may or may not be detected after 30 seconds to 4 minutes. Different algorithms are utilized by the range of available brands and models of patient monitoring equipment.
In this situation, we recommend customers use the FBC MPS450 Multi-Parameter Patient Simulator's VFIB selection with a broader frequency spectrum simulation signal recognizable by the SpaceLabs Healthcare UltraView 1500, Datascope Corporation Passport 2 and other brands/models of patient monitoring equipment used throughout the healthcare delivery system.
The part number for the DataSim 6100 charger is 2184111.
If the probe can physically fit over the Index 2 Test Finger, the probe can be used during testing.